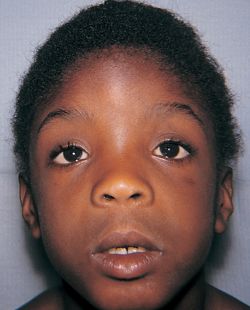
Fetal alcohol
syndrome

http://media18.onsugar.com/files/2011/08/34/2/192/1922664/d5a77cf406fa1a5e_postimfetal-alcohol-syndrome-quiz.jpg
http://media18.onsugar.com/files/2011/08/34/2/192/1922664/d5a77cf406fa1a5e_postimfetal-alcohol-syndrome-quiz.jpg
Fetal alcohol syndrome is growth, mental, and physical problems
that may occur in a baby when a mother drinks alcohol during pregnancy.
Causes
Using alcohol during pregnancy can cause the same risks as using
alcohol in general. But it poses extra risks to the unborn baby. When a
pregnant woman drinks alcohol, it easily passes across the placenta to the
fetus. Because of this, drinking alcohol can harm the baby's development.
There is no "safe" level of alcohol use during
pregnancy. Larger amounts of alcohol appear to increase the problems. Binge
drinking is more harmful than drinking small amounts of alcohol.
Timing of alcohol use during pregnancy is also important.
Drinking alcohol is likely most harmful during the first 3 months of pregnancy.
But drinking alcohol any time during pregnancy can be harmful.


http://www.intellectualdisability.info/diagnosis/images-1/diagnosis/FAS_Face.jpg
Symptoms and Behaviors
Early Childhood (1-5 yrs.)
• Speech or gross
motor delays
• Extreme tactile
sensitivity or insensitivity
• Erratic sleeping
and/or eating habits
• Poor habituation
• Lack of stranger
anxiety
• Rage
• Poor or limited
abstracting ability (action/consequence connection,
judgment &
reasoning skills, sequential learning)
Elementary years
• Normal,
borderline, or high IQ, but immature
• Blames others for
all problems
• Volatile and
impulsive, impaired reasoning
• School becomes
increasingly difficult
• Socially isolated
and emotionally disconnected
• High need for
stimulation
• Vivid fantasies
and perseveration problems
• Possible
fascination with knives and/or fire
Adolescent years (13-18 yrs.)
• No personal or
property boundaries
• Naive,
suggestible, a follower, a victim, vulnerable to peers
• Poor judgment,
reasoning, and memory Isolated, sometimes
depressed and/or
suicidal
• Poor social skills
• Doesn't learn from
mistakes
Educational Implications
Children
with FASD need more intense supervision and structure than other children. They
often lack a sense of boundaries for people and objects. For instance, they
don't 'steal' things, they 'find' them; an object 'belongs' to a person only if
it is in that person's hand. They are impulsive, uninhibited, and
over-reactive. Social skills such as sharing, taking turns, and cooperating in
general are usually not understood, and these children tend to play alongside
others but not with them. In addition, sensory integration problems are common,
and may lead to the tendency to be high strung, sound-sensitive, and easily
over-stimulated.
Although they can focus their attention on the task at hand,
they have multiple obstacles to learning. Since they don't understand ideas,
concepts, or abstract thought, they may have verbal ability without actual
understanding. Even simple tasks require intense mental effort because of their
cognitive impairment. This can result in mental exhaustion, which adds to
behavior problems. In addition, since their threshold for frustration is low,
they may fly into rages and temper tantrums.
A common impairment is with short-term memory, and in an effort
to please, students often will make up an answer when they don't remember one.
This practice can apply to anything, including schoolwork or behaviors. These
are not intentional 'lies,' they just honestly don't remember the truth and
want to have an answer. Since they live in the moment and don't connect their
actions with consequences, they don't learn from experience that making up
answers is not appropriate.
Instructional Strategies and Classroom
Accommodations
- Be as consistent as possible.
The way something is learned the first time will have the most lasting
effect. Re-learning is very difficult and therefore any change is
difficult.
- Use a lot of repetition. These
students need more time and more repetition than average to learn and
retain information. Try using mnemonics like silly rhymes and songs. Also
have them repeatedly practice basic actions and social skills like walking
quietly down the hall or when to say 'thank you.' Be positive, supportive,
and sympathetic during crises; these are children who 'can't' rather than
'won't.'
- Use multi-sensory instruction
(visual, olfactory, kinesthetic, tactile, and auditory). More senses used
in learning means more possible neurological connections to aid in memory
retrieval.
- Be specific, yet brief. These
students have difficulty 'filling in the blanks.' Tell them step-by-step,
but not all at once. Use short sentences, simple words, and be concrete.
Avoid asking 'why' questions. Instead, ask concrete who, what, where, and
when questions.
- Increase supervision - it
should be as constant as possible, with an emphasis on positive
reinforcement of appropriate behavior so it becomes habit. Do not rely on
the student's ability to 'recite' the rules or steps.
- Model appropriate behavior.
Students with FASD often copycat behavior, so always try to be respectful,
patient, and kind.
- Avoid long periods of deskwork
(these children must move). To avoid the problem of a student becoming
overloaded from mental exhaustion and/or trying to sit still, create a
self-calming and respite plan.
- Post all rules and schedules.
Use pictures, drawings, symbols, charts, or whatever seems to be effective
at conveying the message. Repeatedly go over the rules and their meanings
aloud at least once a day. Rules should be the same for all students, but
you may need to alter the consequences for a child with FASD.
- Use immediate discipline. If
discipline is delayed, the student with FASD will not understand why it's
happening. Even if the student is told immediately that a consequence will
happen the next day, he or she will likely not make the connection the
next day. Never take away recess as a consequence - children with FASD
need that break to move around.
- Ensure the student's attention.
When talking directly to the student, be sure to say his or her name and
make eye contact. Always have the student paraphrase any directions to
check for understanding.
- Encourage use of positive
self-talk. Recognize partially correct responses and offer positive
incentives for finishing work. Try to set them up for success, and
recognize successes every day! (or even every hour).
http://www.cmhsreach.org/disorder_fetal.html


http://www.psychiatry.emory.edu/PROGRAMS/GADrug/images/1-79.jpg
https://i.ytimg.com/vi/WfbztgLafPY/hqdefault.jpg
Below is a video going more in depth about Fetal Alcohol Syndrome
https://www.youtube.com/watch?v=j437LKwBEzE
http://www.psychiatry.emory.edu/PROGRAMS/GADrug/images/1-79.jpg
https://i.ytimg.com/vi/WfbztgLafPY/hqdefault.jpg
{kind=link}
Below is a video going more in depth about Fetal Alcohol Syndrome
https://www.youtube.com/watch?v=j437LKwBEzE
Prevalence of FASDs
- We do not know exactly how many people have fetal alcohol spectrum disorders (FASDs). Several different approaches have been used to estimate how many persons are living with FASDs in the population. FASDs include several diagnoses related to exposure of the baby to alcohol during pregnancy. More specifically, fetal alcohol syndrome (FAS) is the most involved diagnosis, used when several physical and developmental abnormalities are present (see Facts about FASDs).
- Using medical and other records, CDC studies have identified 0.2 to 1.5 infants with FAS for every 1,000 live births in certain areas of the United States.1 The most recent CDC study analyzed medical and other records and found FAS in 0.3 out of 1,000 children from 7 to 9 years of age. 2
- Studies using in-person assessment of school-aged children in several U.S. communities report higher estimates of FAS: 6 to 9 out of 1,000 children. 3,4
- Few estimates for the full range of FASDs are available. Based on community studies using physical examinations, experts estimate that the full range of FASDs in the United States and some Western European countries might number as high as 2 to 5 per 100 school children (or 2% to 5% of the population).3,4
Cost of FASDs
- The lifetime cost for one individual with FAS in 2002 was estimated to be $2 million. This is an average for people with FAS and does not include data on people with other FASDs. People with severe problems, such as profound intellectual disability, have much higher costs. It is estimated that the cost to the United States for FAS alone is over $4 billion annually.

http://www.slate.com/content/dam/slate/blogs/moneybox/2014/10/24/find_unclaimed_property_check_these_sites_to_see_if_somebody_owes_you_money/109471093-currency-is-seen-in-this-january-30-2001-image-afp.jpg.CROP.promo-mediumlarge.jpg
Below are more accommodations/strategies that can be used in the classroom when dealing with children with Fetal Alcohol Syndrome.
Teaching Strategies
- Learn about FASD – to understand the condition and impact on learning and behaviour.
- Talk with parents and carers – as they are often experts on their child and will know particular strengths and which developmental areas have been most affected by FASD. They will often know what strategies work (and do not work) for their child.
- Structure and routine – are crucial for a child with neurodevelopmental disorders. This is essential to reduce anxieties and allow the child a sense of predictability while learning.
- Support – FASD-driven adaptations in the same way as you would a pupil with a physical disability by providing support in both the classroom and playground.
- Adapt the environment – to best suit the child’s learning style and ability.
- Think younger – according to the child’s developmental stage (not chronological age).
- Supervise – as you would a younger child. Children and adolescents with FASD are usually trusting and friendly but lack the ability to discriminate between a genuine friend and someone who might harm them. Safety is paramount for those responsible for a child or adolescent with FASD.
- Strategies – to deal with dysmaturity and challenging behaviours. Recognise that the child is behaving appropriately for their developmental age, which is often less than their chronological age.
- Avoid sensory and cognitive overload – by employing calming strategies and time-out. Maintain low stress environments where possible.
- Strengths – every child with FASD has a unique set of strengths e.g. creativity, artistic ability and helpfulness. Identify and build skills and competencies around these and watch the child bloom and grow.
- Life skills – normally learned indirectly by observation and experience need to be taught specifically to those affected by FASD. Tuition on life skills should include advice on planning time, managing money and keeping safe.
- Teamwork – You will not be able to do it all on your own. You will need to join other professionals and parents to form multidisciplinary teams.
http://enquire.org.uk/features/education-of-children-affected-by-fetal-alcohol-spectrum-disorders

http://www.paymystudentloans.com/wp-content/uploads/2012/09/Loan-Forgiveness-For-Teachers.jpg